
FACTS ABOUT LATE-TERM ABORTIONS IN THE U.S.
Updated August 2024
Operation Rescue defines “late-term abortion” as any abortion done in the second or third trimester (about 14 weeks gestation or later), when the baby has grown too large for first trimester procedures like abortion-inducing drugs or aspiration.
A survey of all abortion facilities in the U.S. is conducted annually by Operation Rescue. The data from these surveys offers the most up-to-date and accurate information available, including the number of facilities that offer late-term abortions.
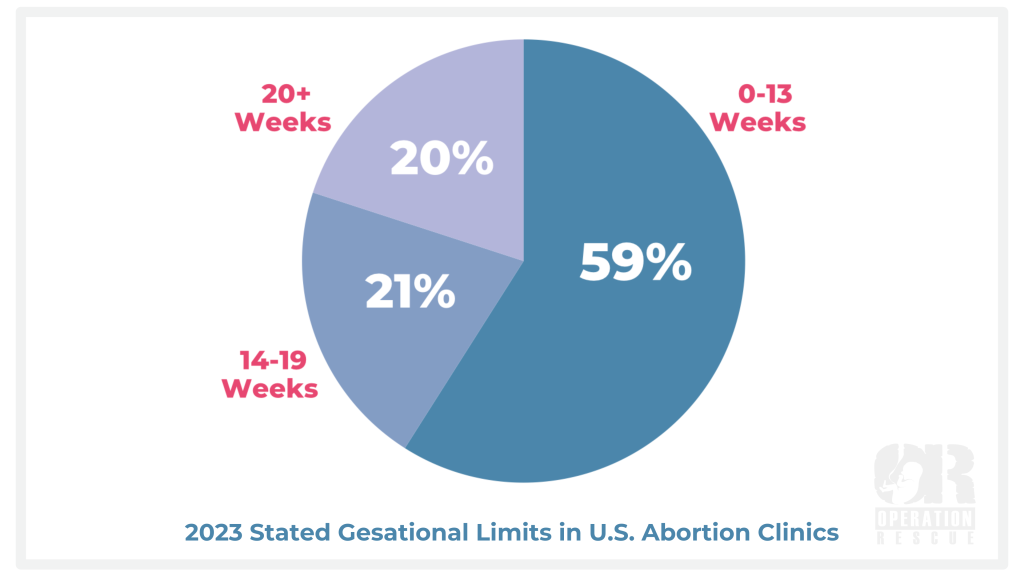
According to our most recent survey, clinics that perform abortions after 20 weeks gestation rose from 16% in 2022 to 20% in 2023. Twenty-one percent of all clinics perform abortions between 14 and 19 weeks gestation.
In total, 41% of abortion clinics in the U.S. currently perform late-term abortions.
A recent study from the Charlotte-Lozier institute confirms that late-term abortion is also available in the United States for any reason. The study refers to elective late-term abortion – not the imagined medical emergencies or dire situations that abortion lobby constantly trots out.
Out of 193 U.N. countries, only eight allow elective abortion on demand through all nine months. America is tragically on that list, aligning our nation with countries like China, which is infamous for using forced abortion to intimidate and control citizens.
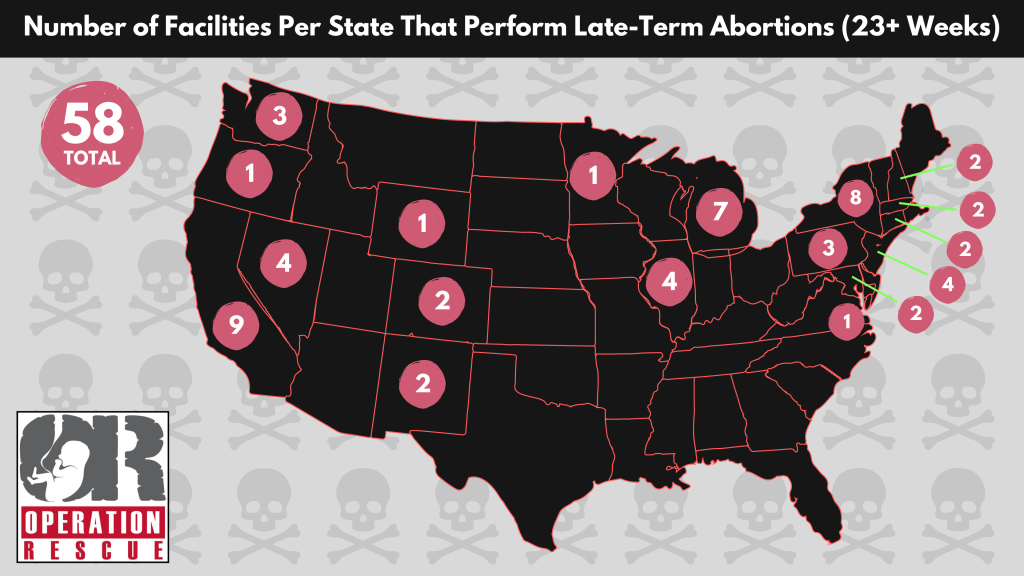
Operation Rescue also recently conducted a survey to identify how many abortion facilities in America offer abortion at 23 weeks and beyond – 23 weeks being far into the second trimester, when the baby’s heartbeat is loud enough to hear through a stethoscope and her lungs and body developed enough to possibly survive outside the womb with modern medical interventions. The total is 58 facilities across 18 states.
Abortion facilities that offer abortions throughout all stages of pregnancy are open about having no gestational limits. Others may state limits under the third trimester of pregnancy even though they actually will conduct them much later. Abortion facilities with “fetal indications” programs, or that conduct abortions for other so-called “medical” reasons, have essentially stripped away all stated gestational limits.
Currently, eight abortion facilities openly abort in the third trimester. It is likely other abortionists commit abortions this late into pregnancy, but are more secretive about it. The current list of eight clinics includes:
- Boulder Abortion Clinic | Boulder, CO
- Stated limit: 30 Weeks (No longer does first trimester abortions)
- Washington Surgi-Clinic | Washington D.C.
- Stated limit: 29 Weeks
- Hope Clinic For Women | Granite, IL
- Stated Limit: 28 Weeks
- C.A.R.E. | Bethesda, MD
- Stated limit: 35 Weeks
- Partners in Abortion Care | College Park, MD
- Stated Limit: 34 Weeks
- Cherry Hill Women’s Center | Cherry Hill, NJ
- Stated Limit: 29 Weeks
- Southwestern Women’s Options | Albuquerque, NM
- Stated limit: 28 Weeks (and beyond – “fetal anomaly” program that offers no gestational limits)
- DuPont Clinic, Washington, D.C.
- Stated limit: 32 Weeks
THE PROCESS: INDUCTION ABORTION (AKA THE “M.O.L.D TECHNIQUE”)
The induction abortion, with the use of a Digoxin injection, was pioneered by late-term abortionist George R. Tiller of Wichita, Kansas. It is now widely used throughout the United States by the few abortionists who are willing to admit they do the late-term procedures. Induction has replaced the live partial-birth abortion method since 2007, when the Partial Birth Abortion Ban Act was upheld by the U.S. Supreme Court.
In videos obtained by Operation Rescue, Tiller is seen describing this particular abortion method, known as the M.O.L.D. Technique, which is an acronym for the four products employed in the abortion process: Misoprostol, Oxytocin, Laminaria, and Digoxin.
Currently, this late-term abortion process is used in pregnancies as late as 35 weeks. It is used when the baby grows too large to make dismemberment (Dilation & Evacuation, or D&E) abortions impractical due to the calcification of bones and development of ligaments and musculature in the growing baby’s body.
“We think the process is safe. Nothing is perfect.” – George Tiller
The induction abortion takes 3-4 days to complete.
On the first day, the woman is given an ultrasound to determine the gestational age of her baby. Then, with the aid of the ultrasound to guide the abortionist, a lethal dose of the heart medication Digoxin is injected into the baby’s heart or into the amniotic fluid directly through the woman’s abdomen. (Potassium chloride is infrequently substituted for Digoxin.) Digoxin gives the baby a fatal heart attack. This is an off-label application of the drug, which was originally developed and approved as a treatment for heart disease. In some cases, the injection can be made vaginally instead of through the abdomen.
In a video shown to abortion patients, Tiller discusses the fatal injection:
“Although you may find this a little difficult and a little uncomfortable, on the first day that you arrive at the clinic we will make an injection of a medication called digoxin into the fetus to initiate fetal demise.”
Tiller elaborates on his reasons for killing the baby before beginning the surgical abortion procedure.
“The first reason is so that there will be no fetal pain. We — we have learned with hundreds and hundreds and hundreds of patients that women have the question about, ‘Will this be painful for our baby? Will this be painful for my baby?’ And the answer to that is, ‘No.’ We make an injection directly into the fetus with a medication called digoxin on the day that you arrive so that the baby will expire painlessly. The first reason is no fetal pain.”
However, those who have experienced massive heart attacks, describe them as extremely painful and frightening. It is well documented that babies in the later stages of pregnancy can feel pain, and more recent studies confirm babies as young as 6-8 weeks gestation may experience pain.
While the concept that a late-term baby can feel pain is often disputed in the press and by abortion supporters, it is obvious that Tiller believed that late second and third trimester pre-born babies can feel pain, and thus used his lethal fetal injection as a means of allaying the concerns of abortion patients.
However, the more crucial (and brutal) reason for killing the baby first is to avoid a live birth. This prevents a myriad of problems for the abortionists, including running afoul of state and federal laws protecting the life of the baby after a live birth, even if the birth is the result of an abortion.
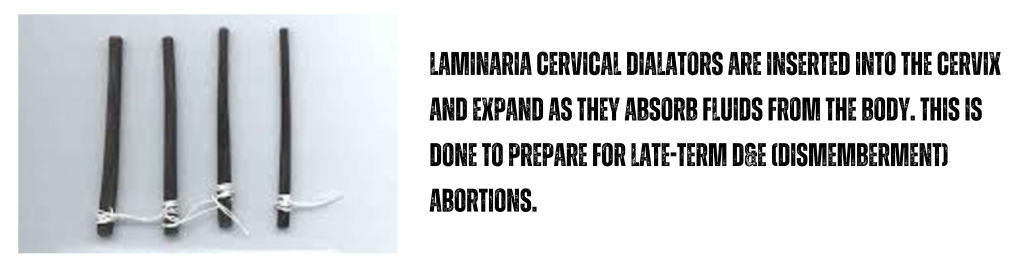
After the Digoxin injection, the woman’s cervix is packed with laminaria, thin tampon-like sticks made of seaweed that expand the cervix gradually over the next day. The drug Misoprostol is also administered vaginally to “ripen” the cervix for the upcoming delivery of the dead baby.
Misoprostol is a drug that was originally manufactured to treat stomach ulcers. Its use in abortions is an off-label application, stimulating uterine contractions which are unpredictable and sometimes violent.
After the first day’s injection and cervical preparation, the patient is sent home or to a local hotel where she will remain unmonitored until her appointment at the clinic the following day.
On day 2 of the procedure, the woman is repacked with even larger laminaria sticks and given additional Misoprostol to prepare the woman for labor. The Misoprostol may be administered both vaginally or buccally (between the cheek and jaw), depending on whether delivery is expected on day 3 or 4. If the woman is undergoing a later, four day process, she will return on day 3 for additional laminaria and Misoprostol. Each day until delivery, she is sent back to her hotel where she remains unmonitored, even though active labor has begun or is in progress.
Because of this lack of monitoring, women sometimes cannot get to the clinic in time and deliver their dead babies in the hotel, in vehicles, or other places where medical assistance is nonexistent. Tiller admitted as much in a video he produced for the purpose of introducing prospective abortion patients to the late-term abortion process.
“At Women’s Health Care Services, our late elective abortion program involves managing the pregnancy by the premature delivery of a stillborn.” – George Tiller
On the final day of the abortion, the woman is given the drug Oxytocin, which induces or augments contractions and the onset of labor. Women are then placed in a room where they endure the final stage of the labor process. When it is determined that the labor has progressed to the point where the baby is about to be delivered, each woman is usually taken into a room with a toilet and told to lean on the nurse and push the baby into the toilet.
The toilet delivery method has been used by a number of abortionists, including Florida abortionist James Pendergraft. Other abortionists may allow the woman to deliver on a delivery table. Still others, such as former Michigan abortionist Alberto Hodari, prefer to remove the dead baby through dismemberment.
Once the dead baby is delivered, the woman is given a procedure called Dilation & Curettage, or D&C. Here, a sharp edged spoon-shaped instrument is used to remove the remaining tissue, such as the afterbirth, from the uterus.
After the abortion, or the following day, the woman is given what Tiller’s employees called the “Party Pack,” which includes abortion aftercare instructions and a prescription for birth control pills. They are then released to return home.
Other abortionists have responded publicly to the increased use in the Induction abortion with digoxin injection method and its dangers.
The now retired Michigan abortionist Alberto Hodari preferred to dismember live babies between 18 and 24 weeks. He told the Detroit News on July 30, 2007, “It was much simpler and much less dangerous than what we are doing now. But this is now the law. It’s awful. It’s unnecessary. It’s dangerous. It’s more complicated. It makes the woman go through another procedure that’s not necessary. It impacts everything we do after 18 weeks.” Hodari began using the injections even though he considered them dangerous.
“We do not believe that our patients should take a risk for which the only clear benefit is a legal one to the physician,” abortionist Philip D. Darney, Director Emeritus told the Boston Globe in 2007 at the Bixby Center for Global Reproductive Health, which pushes a depopulation agenda around the world. He chose not to use the injections.
Complications from lethal fetal injections are well known. In Orlando, Florida, the misuse of Digoxin resulted in the live birth of Baby Rowan, who died after abortion clinic workers denied him medical care.
In Wichita, Kansas, Tiller’s needle slipped, and Baby Sarah was injected in the head with a toxic drug that was a precursor to Digoxin. She survived and was later adopted, but suffered a malady of medical problems. She died five years later from complications to the injuries she received as a result of the injection.
Operation Rescue Senior Vice President Emeritus Cheryl Sullenger states, “Frankly, debate over Digoxin and dead baby abortions versus live baby abortions is absurd. The result is still a dead baby. Both procedures are barbaric and hold serious risks to women. The act of killing a pre-born baby is in itself immoral and until we can come to grips with that as a society, we will never be able to value life as we should.”
MOST AMERICANS OPPOSE LATE-TERM ABORTIONS
According to polls as recent as 2023, the majority of Americans do not support abortion in the second or third trimester, yet abortion remains available in our nation though all nine months and protected by our federal government.
A Gallup poll published in June 2023 showed that 55% of Americans oppose abortion in the second trimester and 70% oppose it in the third trimester.
In June 2021, an AP-NORAC poll noted that for pregnancies in the second trimester, 65% of Americans said that abortion should be illegal in most or all cases, and 80% said abortions in the seventh, eighth, and ninth months of pregnancy should be illegal in most or all cases.
RISKS INCREASE WITH LATE-TERM ABORTIONS
Women also run additional risks when submitting to this abortion procedure. For every week that passes, the abortion risks to a woman’s health and life increase.
One woman suffered a ruptured uterus during a 35-week abortion done by Shelley Sella in Albuquerque, New Mexico. Sella ignored the patient’s medical history of a previous Cesarean Section delivery, for which the use of Misoprostol is contraindicated. Sella was charged by the New Mexico Medical Board for gross negligence in this case, but escaped punishment.
Christin Gilbert, 19, and Jennifer Morbelli, 29, died from complications to third-trimester abortions done by LeRoy Carhart. Both women suffered a complication known as disseminated intravascular coagulation (DIC), a blood clotting disorder that leads to massive hemorrhage. Gilbert may also have suffered from sepsis, a live-threatening blood infection. Morbelli’s complications included an amniotic embolism, which is a treatable condition if caught in time.

There is rising concern that the entire induction process as practiced by Sella, Carhart, and others, is too dangerous for use in outpatient clinics since women who have begun the surgical abortion process are left unmonitored outside the clinic for long periods of time without access to immediate emergency care.
Dr. Gerald L. Bullock, a Texas Obstetrician and Gynecologist considered an expert in the field, has expressed his professional opinion that the process violates the standards of patient care because it fails to follow the accepted protocols set forth by the American Congress of Obstetricians and Gynecologists.
In 2020, a whistle-blower from a local hospital came forward to describe two women who received late-term abortions at LeRoy Carhart’s C.A.R.E. clinic in Bethesda, Maryland — one on May 12, 2020, and the other on May 21, 2020. Both women, who were both 25 weeks pregnant, suffered from large holes torn in their wombs during the abortions. Both were hospitalized for several days, underwent emergency surgery, and received multiple units of blood to save their lives. [Read the full report substantiating documents.]
According to the whistleblower, those involved in treating the woman involved in the medical emergency on May 12 were so upset by what they saw that the surgeon felt the need to send an e-mail to the hospital staff acknowledging their trauma while caring for this woman.
This same hospital worker described the injuries to the second woman who was hospitalized on May 21, 2020, as “the most horrific thing I have ever seen.”
Don’t let this happen to you. If you’re pregnant and need help, please click the link below. There are many loving people waiting to help you!

Related resources:
New Mexico Medical Board Disciplinary Hearing Transcripts in the case of Shelley Sella, November 29-30, 2012:
